My name is Dianna McAllister and I am approaching the finish of my second year at University of Toronto, pursuing a bioinformatics specialist and computer science major. This year I was given the incredible opportunity to work in Dr. Tyrrell’s lab for the ROP299 course.
I have just handed in my first ever formal research paper for my work in Dr. Tyrrell’s lab. My project observed the effectiveness of using grad-CAM visualizations on different layers in a convolutional neural network. Though the end results of my project were colourful heat maps placed on top of images, the process to get there was not nearly as colourful or as effortless as the results may seem. There was lots of self-teaching, debugging, decision-making and collaboration that went on behind the scenes that made this project difficult, but much more rewarding when complete.
My journey in Dr. Tyrrell’s lab began when I first started researching ROP projects. I can still remember scrolling through the various projects, trying to find something that I thought I would be really passionate about. Once I happen upon Dr. Tyrrell’s ROP299, I could feel my heart skip a beat- it was exactly the research project that I was looking for. It explained the use of machine learning in medicine, specifically medical imaging. Being in bioinformatics, this project was exactly what I was looking for; it integrated biology and medicine with computer science and statistics. Once I saw this unique combination, I knew that I needed to apply.
After I applied, I was overjoyed that I had received an interview. When I attended the interview, I was very excited to show Dr. Tyrrell my interest in his research and explain how my past research would help me with this new project. But once I walked into his office, it was unlike any other interview I had ever had; he was able to point out things about myself that I had barely even realized and asked me many questions that I had no answer to. I remember walking out of that interview feeling disappointed as I thought that there was no way I would get a position in his lab, but a few weeks later heard back that I had gotten the position! I was delighted to have the opportunity to prove to Dr. Tyrrell that he made a good choice in choosing me for the position and that I would work hard in his lab and on my project.
The night before my first lab meeting, I researched tons of information on machine learning, making sure to have- what I thought- an in-depth understand of machine learning. But after less than five minutes into the lab meeting, I quickly realized that I was completely wrong. Terms like regression, weights, backpropagation were being thrown around so naturally, and I had absolutely no idea what they were talking about. I walked out of the meeting determined to really begin understanding what machine learning was all about!
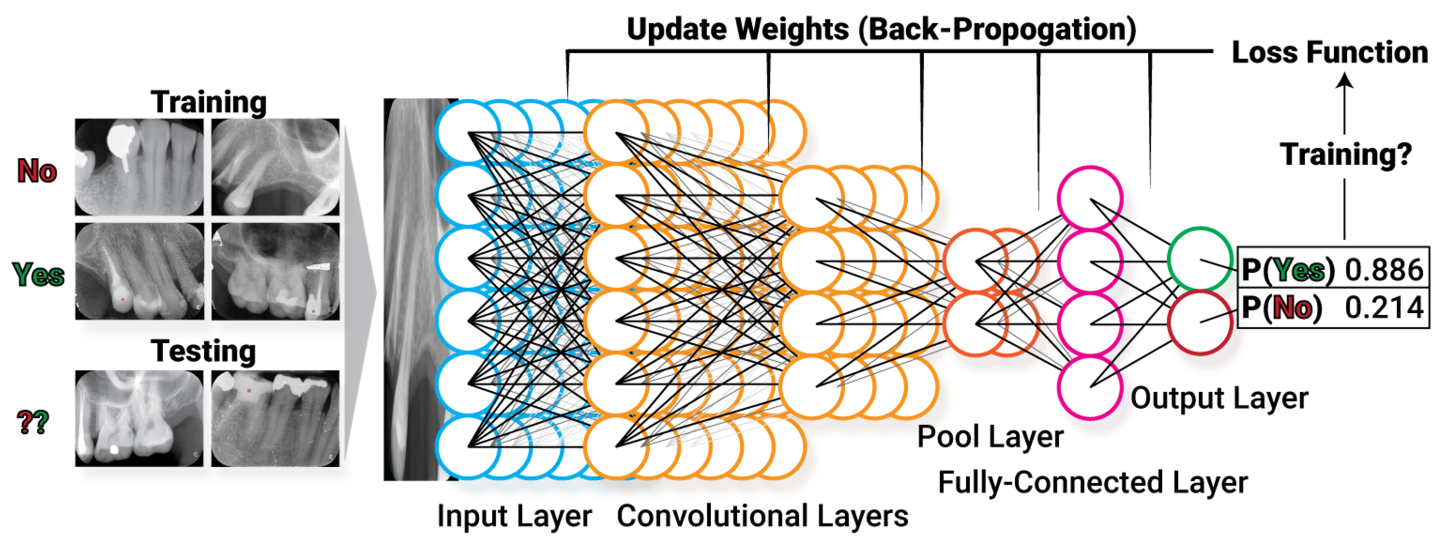
Thus began my journey to begin my project. When I decided on my project, it seemed fun and not too difficult- all I have to do is slap on some heat maps to images, right? Well as much as I felt it wouldn’t be too difficult, I was not going to be deceived just as I had before attending our first meeting; and after completion I can definitely say it was not easy! The first problem that I encountered immediately was where to start. Sure, I understood the basic concepts associated with machine learning, but I had no experience or understanding of how to code anything related to creating and using a convolutional neural network. I was fortunate enough to be able to use Ariana’s CNN model. Her model used x-rays of teeth to classify if dental plates were damaged and therefore adding damage (artifacts) to the x-rays of teeth or if the plates were functional. It took me quite some time to understand what each line of code did within the program- the code was incredible, and I could not imagine having to write it from scratch! I then began the code to map the grad-CAM visualizations (resembling heat maps) onto the images that Ariana’s model took as input. I was again fortunate enough to find code online that was similar to what I needed for my project. I made very minor tweaks until the code was functional and worked how I needed it to. Throughout this process of trying to debug my own code or figure out why it wouldn’t even begin running, Mauro was always there to help, always being enthusiastic even when my problem was as silly as accidentally adding an extra period to a word.
Throughout the process, Dr. Tyrrell was always there as well- he always helped me to remember the big picture of what my project was about and what I was trying to accomplish during my time in his lab. This was extremely valuable, as it kept me from accidentally veering off-course and focusing on something that wasn’t important to my project. Without his guidance, I would have never been able to finish and execute the project in the way that I did and am proud of.
Everything that I learned, not only about machine learning, but about how to write a research paper, how to collaborate with others, how to learn from other’s and your own mistakes and how to keep trying new ideas and approaches when it seems like nothing is working, I will always carry with me throughout the rest of my undergraduate experience and the rest of my professional future. Thank you, Dr. Tyrrell, for this experience and every opportunity I was given in your lab.
Dianna McAllister